
Browsing Øystein Horgmo’s blog about medical videography (see earlier post here) I also fell over his description of the sounds of the operating room.
The auditory space is one of those forgotten dimensions of medical science studies (see an earlier post here). As far as I remember, I haven’t seen any historical work on contemporary medicine or any medical science studies project that pays attention to the medical soundscape.
That’s a shame, because the hearing sense is more open for presence-effects (á la Gumbrecht) than vision. In other words, the auditory qualities of the medical world is a potentially very interesting sensory dimension for curators of medical museums to work with.
Here is Øystein’s description of the sounds of the operating room (my underline of auditory indicators; wish he had put an mp3-file on his blog instead of putting it in words!):
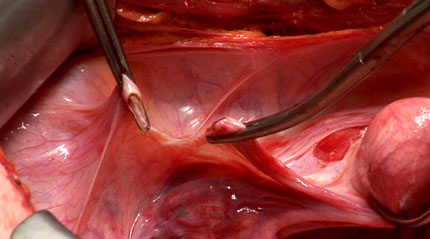
Below all the other sounds is the constant, but barely audible hiss of the ventilation. This is especially strong and effective in ORs, to keep the air as clean as possible. Slightly above lies the perpetual mechanic breathing of the respirator. Adding to this basis is the more prominent, but still subtle machine hum of the suction pump. It’s a sound you don’t notice till it’s gone. Nothing creates a calm atmosphere like turning off the suction. Against this constant background noise comes the busy but calm sounds of the actual surgery. The clanking of steel against steel as the scrub nurse puts instruments back on the back table. The high pitched tone from the electrocautery unit when the surgeon steps on the remote pedal. The characteristic two or three clicks of the toothed locking mechanism as a clamp is closed. The slurping sound of the suction in use. And around all this, the murmur of the surgical team. The scrub and circulating nurses exchanging equipment and counting sponges. The surgeon calling for instruments and ordering the assistant. The laughs. The small talk. This steady rhythm is broken now and then by the occasional blips of the surgeon’s pagers (left by the entrance), ringing of the intercom and the insistent beeping of the anesthetist’s monitors. And that’s about it. The aural atmosphere of the OR.
I’m already imagining up a museological research project on the representation of medical soundscapes in collections and displays. Anyone out there who would like to work with us on this topic?


 And there are
And there are  (
( (
(
 (
(